| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
616 Theories and techniques of oral implantology
Because the vent-plant is self-tapping, it is screwed directly into the bone to the desired depth. The blade-vent is tapped to its proper depth with a mallet; thus, the implant makes its own path in bone. However, mistakes do occur (Fig. 14-16) .
Lack of parallelism. Implants should be seated so that they are parallel to each other and to the remaining prepared teeth. When they are not set into the bone so that they are perpendicular to the occlusal plane or in a direct line parallel to the occlusal forces, they will not be able to withstand the masticatory pressures brought to bear upon them (Fig. 14-17). Also, it is very difficult to fabricate a fixed partial or complete bridge that will fit passively over nonparallel posts. Telescopic copings may be used, but it is better to avoid this complication.
Insufficient number of implants or natural teeth. Any structure, natural or man-made, needs a strong enough foundation to stabilize it. This is particularly true when dealing with the number of implants needed to support a full arch fixed denture. For example, if sufficient alveolar bone exists only in a few scattered areas of an edentulous maxilla or mandible and only a few implants can be placed, in time the case will fail (Fig. 14-18). If five or six implants are indicated and if there is alveolar bone
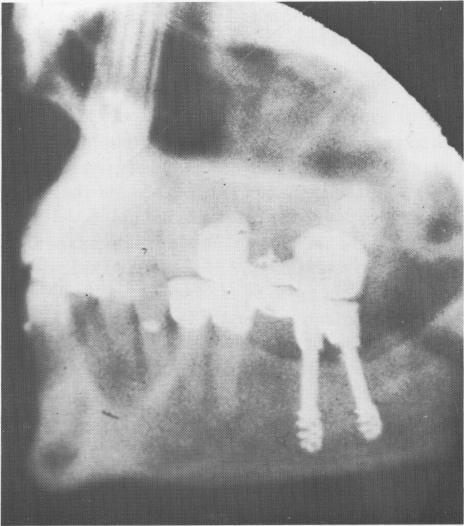
Fig. 14-14. The spiral-shaft implants were set through and below the inferior border of the mandibular canal, causing a paresthesia.
available for only three, it is obvious that the three cannot do the job as well.
The positions of the implants are also important. They must be functionally spaced across the span, not clumped together (Fig. 14-19). When situations arise where clumping of implants or using too few is the only solution, the entire case may be contra-indicated. Frequently, however, a combination of endosseous and subperiosteal implants can success-fully solve the problem.
Improper placement of triplant pins. There are very few areas of bone in either the maxilla or man-
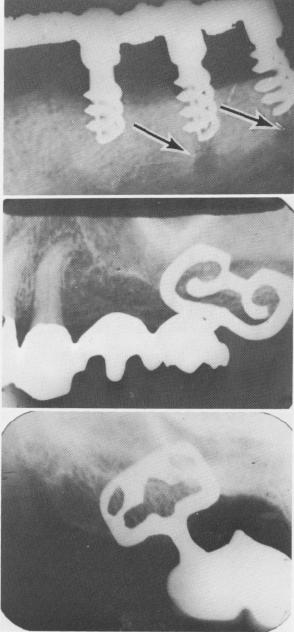
Fig. 14-15. A, Failure of implants resulted from the fact that the implants met too much resistance from the bone and therefore could not be screwed as deeply as the pre-ceding bone burs. As a result, the spirals were not buried deep enough under the fibromucosal tissue, which led to bone resorption. (From Linkow, L. I.: Alloplastic implants. In Goldman, H. M., Forrest, S. P., Byrd, D. L., and Mc-Donald, R. E.: Current therapy in dentistry, vol. 3, St. Louis, 1968, The C. V. Mosby Co., pp. 335-356.) B and C, Although sufficient bone existed, a portion of the shoulders of each one of the blade implants was not buried under the alveolar crest. Although these implants are still functioning satisfactorily in the mouth, this error could lead to failure.
A
B
C
|
|
Page 616 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|